

The Long & Short Of It (LV Function)
- FOAMfrat

- Oct 13, 2021
- 5 min read
Anyone who follows me on social media knows how big of a fan of ultrasound I have become since working at Life Link III. It's been over four years of scanning for me, and in my opinion, the cardiac ultrasound is the exam that has impacted my treatment the most (lung ultrasound is a close second). In this blog, I want to introduce you to a few of my favorite ultrasound views and how I use them to obtain more data on left ventricular function..

The Parasternal Long
This view is probably one of the easiest views to obtain and provides you with quite a bit of information. Let's first talk about how to obtain it.
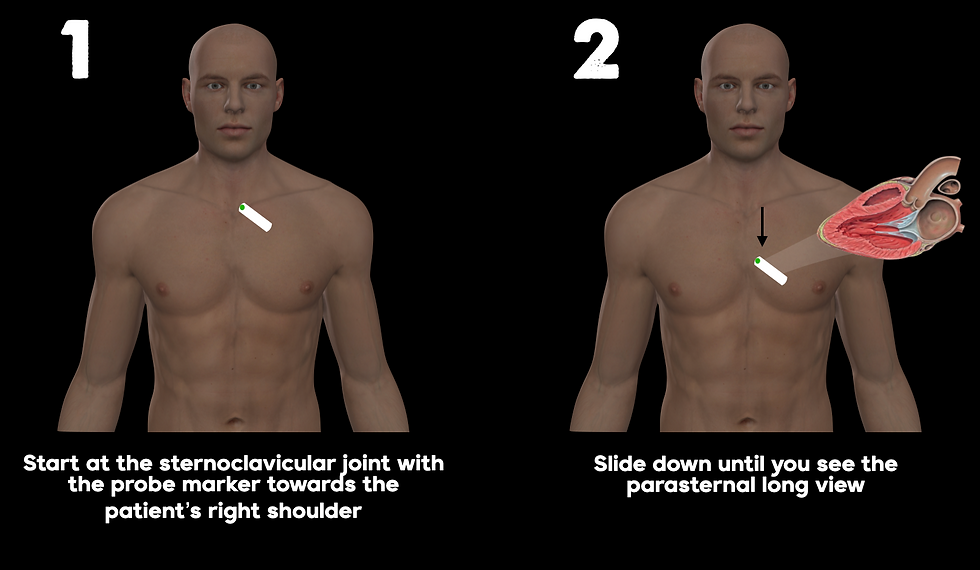
The goal of this view is to slice the heart along its long axis. Instead of just trying to put the probe right over the heart and move it around until you have the right angle, I find it is easier to start at the sternoclavicular notch, with the probe marker pointed toward the right shoulder, and then slowly move down until you see the heart. The reason you tilt the probe at an angle is that the heart is positioned at an angle. If you want to slice it down the long axis, your probe will have to be angled as well. Start sliding your probe down parallel to the sternum, once you see the heart beating, all you have to do is rotate the probe until you see the textbook parasternal long view. It should look something like this.

What are we looking at? Well, you are a fly on the lateral wall and you are looking at the relationship between the left atrium and the left ventricle. This relationship tells us so much about cardiac output and once you train your eye, you will be making clinical decisions in no time.
So we have to get a little nerdy for a second, but I promise it isn't that bad. Imagine a left ventricle full of blood and ready to eject that blood into the aorta. The ventricle contracts and you eject like 70% of that blood out to the body. For a moment, because you got rid of all that volume, your pressure is actually less than your upstairs neighbor, the left atrium. Because of that nice pressure gradient, the mitral valve swings open up like those old saloon doors in western movies and allows the blood from the atrium to fill you up for the next beat.

Now for another scenario. Imagine a left ventricle full of blood and ready to eject that blood into the aorta, the myocytes contract and you eject like 10% of that blood out to the body. The pressure gradient between the left atrium and left ventricle is now significantly reduced. This means that the mitral valve will like barely swing open.

In both of these scenarios, the amount of "swing" we get out of the mitral valve correlates with how much blood we eject during systole. You can see the LV is dilated and that means at the end of systole, there just isn't that much of a pressure gradient between the left atrium and hence a large separation between the mitral valve and septum. This patient is clearly on the plateau of the Frank-Starling curve and increasing preload will not buy you any more cardiac output.
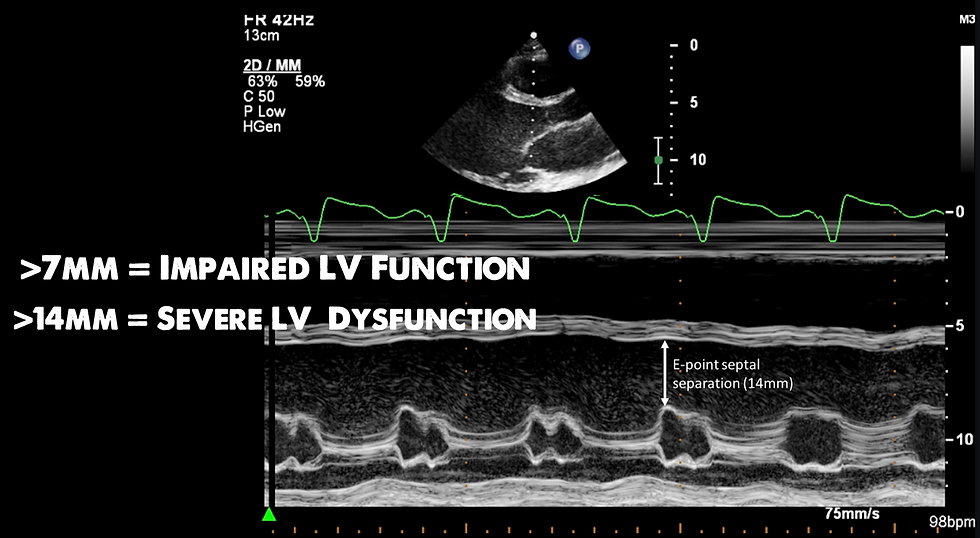
There is a way to calculate this and it is called E-point septal separation. This measures the distance between the mitral valve and septum. If you look at the image below, you will see it is obtained by dropping a motion line across the mitral valve while obtaining a parasternal long view.
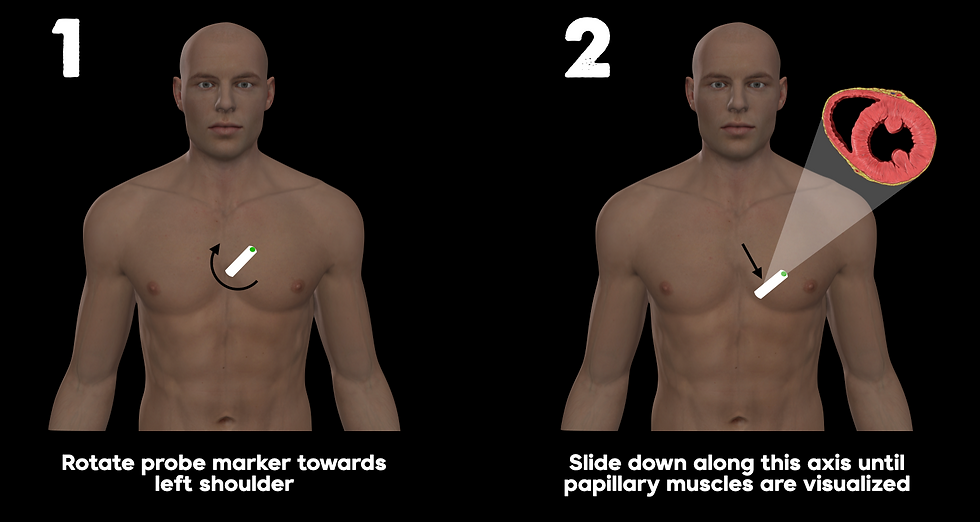
One of the cool things about the parasternal long view is that you can just rotate the probe marker to the left shoulder and obtain a parasternal short view of the left ventricle. This may help better investigate which region is impacting the LV function.
The Parasternal Short
I used to think this view was useless and didn't really tell me much that would impact decision-making. That's because I wasn't looking far enough into it... literally. The parasternal short has a few different ways it slices the LV. I was just looking at the aortic view, which is fine if you are looking for a dissection flap, but if you are looking for wall motion abnormalities, you gotta keep sliding down.
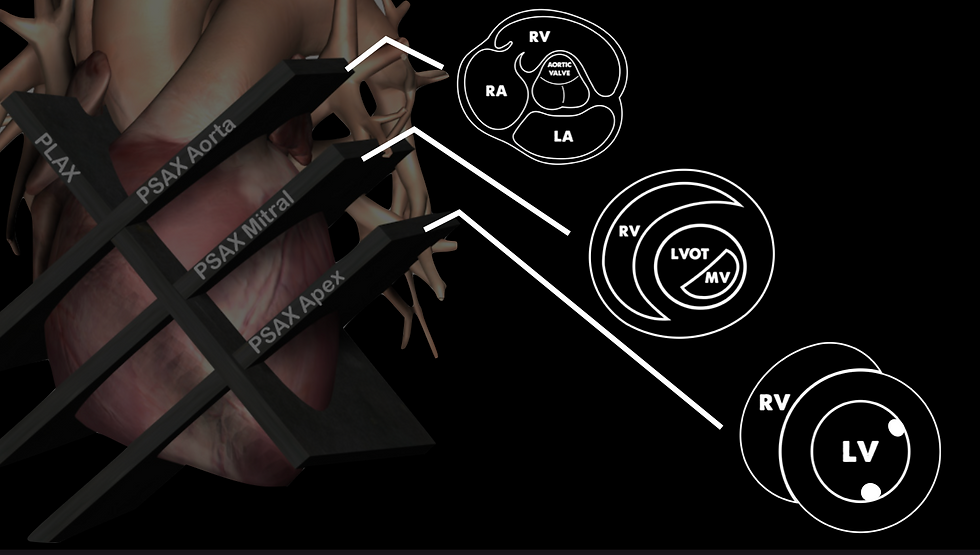
Once you point the probe marker towards the left shoulder, you are now slicing the heart across its short axis. As you move it down, you see the various structures. If trying to identify regional wall motion abnormalities (RWMA) you want to be about mid-ventricle at the level of the papillary muscle.

When you are at the mid cavity of the LV, you will see an image that looks something like this.
Note how you do not see the mitral valves, but rather the papillary muscles (image from the renal fellow network).
I like this view because the regions of the LV actually make sense in my head. The space between the LV and RV is the septum, the bottom of the LV is the inferior portion of the LV, and the anteriorolateral wall is on the right side of the screen.

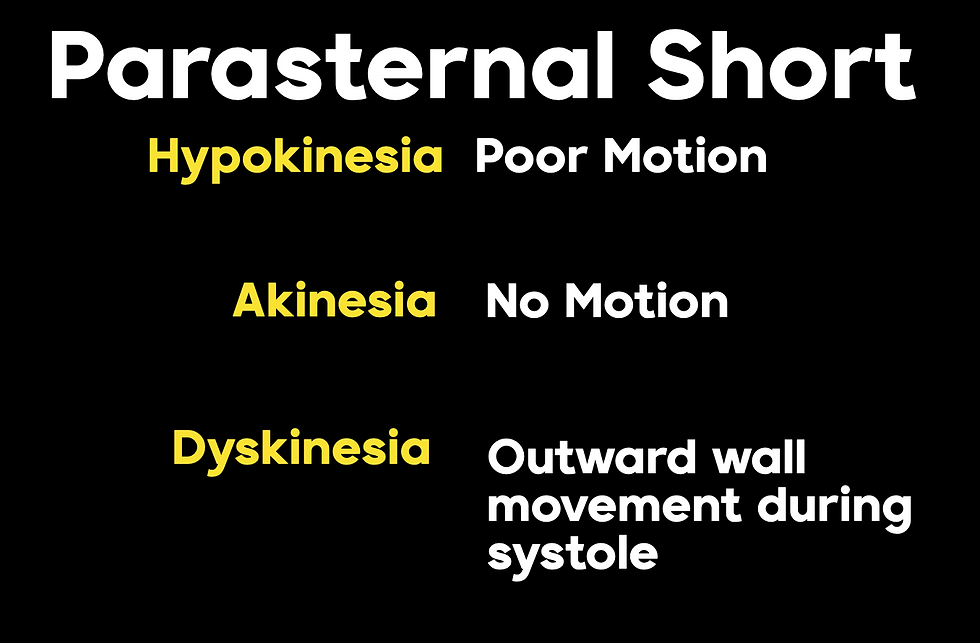
The circumferential shortening of the myocardial fibers will make the walls of the ventricle get fat during systole which decreases the size of the cavity and squeezes out blood into the aorta. If a region of the heart becomes ischemic, the myocardial activity of that region will down-regulate. Check out the image below and see if you can guess which region of the heart the ischemia is coming from.

At first look, you can tell the walls aren't all getting fat and skinny in synchrony. It looks like the inferoseptal region is not moving as much (dyskinesia). If you had minor S-T changes in the inferior leads on your ECG, this would be a nice confirmation. It can be difficult to tell whether the RWMA is old or acute. The scar tissue from myocardial infarction will actually make the ventricle wall thinner and appear brighter on ultrasound.
The nomenclature to describe the activity of a specific cardiac region is actually pretty simple.
There are various reasons for wall motion abnormalities, and just like with any diagnostic test, pre-test probability should hopefully prevent you from going down any rabbit holes. Some of these causes include:
Bundle Branch Block
Pacemaker
Pre-excitation
PVC
RV Strain
Sarcoidosis
Takotsubo Syndrome
It should also be mentioned that if you notice that the wall motion abnormalities involve more than one arterial territory, non-ischemic causes should be considered. Check out this one below and see if you can guess the cause.

If you want to learn more about this topic, check out my webinar I am doing for Philips Lumify, sponsored by Boundtree on October 14th, 2021 at 3 pm EST.

References
Esmaeilzadeh, M., Parsaee, M., & Maleki, M. (2013). The role of echocardiography in coronary artery disease and acute myocardial infarction. The journal of Tehran Heart Center, 8(1), 1–13.
Horowitz RS, Morganroth J, Parrotto C, Chen CC, Soffer J, Pauletto FJ. Immediate diagnosis of acute myocardial infarction by two-dimensional echocardiography. Circulation. 1982;65:323–329. [PubMed] [Google Scholar]
Gerber IL, Foster E. Echocardiography in the coronary care unit: management of acute MI, detection of complication, and prognostic implications. In: Otto MC, editor. The Practice of Clinical Echocardiography. 3rd ed. Philadelphia/China: Elsevier; 2007. pp. 305–315. [Google Scholar]



Comments